Respectfully, Stop Calling Cataplexy “Muscle Weakness”
If you live with Narcolepsy Type 1, you already know the struggle: there is a profound difficulty in the terminology used for all five core symptoms of Narcolepsy. It can be and often is wildly over-generalized and simplified. There is a lack of recognition, familiarity, comprehension of, and difficulty when it comes to discussing Cataplexy.
This discussion isn’t about my individual journey; **it’s about the broader community’s need for evolving terminology that accurately reflects the lived reality of Narcolepsy Type 1**.
Most glaring is the widespread reliance on the term **”muscle weakness”** to define Cataplexy. Frankly, this phrase actively obstructs understanding and “literally exacerbates misunderstanding” of the condition.

Why “Weakness” Fails Us
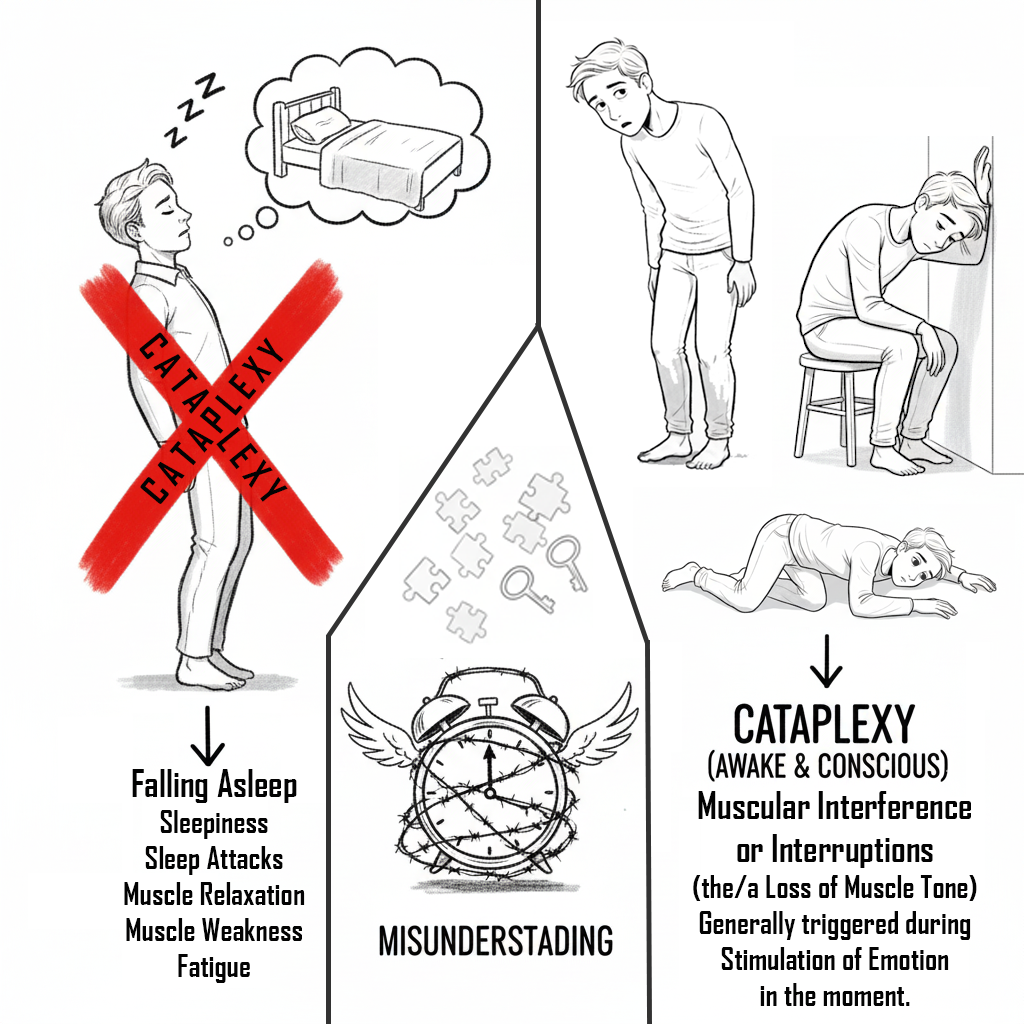
For starters, if you have either type of Narcolepsy, or perhaps Idiopathic Hypersomnia or even a Sleep Apnea matter, you already know what generalized muscle relaxation, fatigue, and well what “muscle weakness” feels like because of sleepiness – living with it, battling it, being up against it on the daily.
Cataplexy, however, is not simply low energy or fatigue. It is a sudden, neurological interruption – a “loss of muscle atonia” – that hits “in the moment” or “fluctuating over ongoing moments” during emotional stimulation and well sure, “muscle weakness” lingers there too.
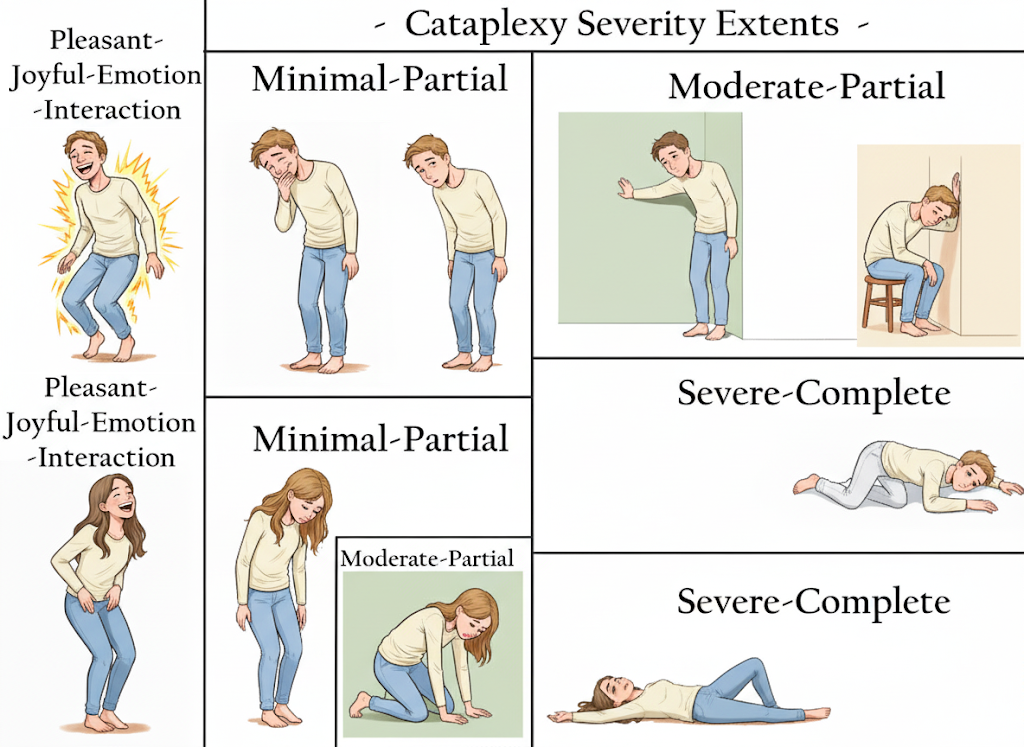
When the clinical definition is so reductive, it risks depersonalizing the entire experience. Calling a profound neurological event “weakness” fails to see the whole person impacted by the symptom. This echoes the disconnect explored by Megan O’Rourke in *The Invisible Kingdom* ( https://youtu.be/S7ovCCIhB_o?si=jA16cWCBdmr7ABvQ ), highlighting how the healthcare system struggles “to see and treat what it cannot easily measure”. Cataplexy runs the gamut from “minimal-partial” to “severe-complete”.
Think about the subtle ways Cataplexy shows up:
A drooping of the jaw, head, or neck. Slouching of the upper torso. A twitching-like loss of facial expression or eye contact. Difficulties with speech. Etc.
Does “muscle weakness” truly capture that range? No.
Can the experience, even the subtle extents be articulated better, more accurately? Yes.
And well, there’s actually still so much more, deeper to Cataplexy.
Interference, Not Weakness
If we want to build a “crucial bridge between the scientific and the human,” we need language that precisely captures the acute, neurological nature of the event. Patient narratives are essential for translating the “cold, objective language of a diagnosis into the personal, emotional, and physical reality of living with an illness”. When terminology is vague, the experience is often dismissed. This is similar to the way Audre Lorde, in *The Cancer Journals* ( https://www.youtube.com/watch?v=wa-jvsgsuXw ), confronted the medical establishment’s tendency to de-personalize the patient.
The replacement term I suggest is **”muscular interference/s and/or interruption/s”**.
This change is not unprecedented. We have historical success in advocacy-driven evolution for other neurological conditions:
* **Autism Spectrum Disorder (ASD):** Advocacy fundamentally transformed the perception of ASD, moving away from harmful psychoanalytic views like the “refrigerator mother” theory and firmly establishing its biological basis.
* **Tourette’s Syndrome (TS):** The patient-led Tourette Syndrome Association shifted the narrative from psychoanalysis to a neurodevelopmental understanding, leading to “more humane and effective care”.
Our struggle is analogous: we must move Cataplexy away from being perceived as a general state of “weakness” or lack of energy – which, let’s be honest, carries its own implicit, harsh stereotypes, like Narcolepsy itself – and firmly redefine it as a specific, acute neurobiological interruption.
By updating the terminology to focus on **”muscular interference/s and/or interruption/s”** alongside “loss of muscle tone,” we gain the necessary clarity to bridge the gap between clinical language and the deeply felt human experience. This evolution is vital if we are to articulate the depth of the condition and ensure that Cataplexy ceases to be a symptom that is “in the dark” while so often misunderstood, and/or straight confused with sleepiness for so many. Helping also in evolving the comprehension towards Narcolepsy, at the same time.
The immense importance of the medical community’s tireless pursuit of scientific clarity, new treatments, and awareness remains foundational, and I reiterate my profound respect for their work.
Disclaimer: The information provided in this article is intended for informational and educational purposes only. Seek a qualified medical professional with expertise in Narcolepsy for diagnosis or treatment. I am not a medical professional.
Spanish version
Japanese/ソロモン・ブリッグスによる日本語訳
Created by: Solomon Briggs
(aka Narcoplexic)
September 23rd, 2025
Bridging The Gap: Evolving Cataplexy & Narcolepsy Terminology © 2025 by Solomon Briggs is licensed under CC BY-NC 4.0
To view a copy of this license, visit https://creativecommons.org/licenses/by-nc/4.0/
“You may use this tool for non-commercial purposes, but must credit Solomon Briggs.”