As Solomon Briggs, an Independent Sleep Advocate with Type 1 Narcolepsy (T1N), I wrote this to address the persistent lack of recognition given to the systemic reality of this neurological system dysfunction. This effort aims to highlight (only a few of what are so many) major facets of the disorder that are routinely unrecognized, dismissed, and downplayed in conventional discourse.
Type 1 Narcolepsy: A Neurological System Crisis
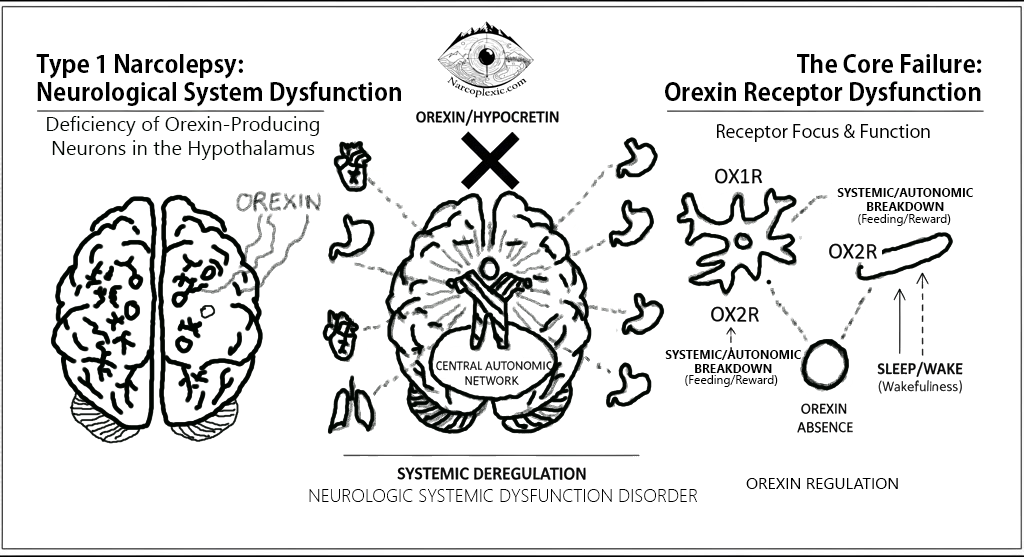
Type 1 Narcolepsy (T1N) is widely mischaracterized as merely a sleep disorder, yet it is fundamentally a neurological system crisis rooted in a deficiency of the critical neuropeptide, Orexin (also known as hypocretin) [1][2]. This deficiency arises from the destruction of orexin-producing neurons in the hypothalamus [2][3][4].
Orexin/Hypocretin normally functions as an excitatory neuropeptide [1] and a key regulator, or “conductor,” within the central autonomic network [2][3]. Even referred to as ‘the conductor of the Orchestra of neurotransmitters, neuropeptides, hormones.’ Its absence causes systemic deregulation across the body, defining T1N as a complex Neurologic Systemic Dysfunction Disorder.
The Core Failure: Orexin Receptor Dysfunction
The disruption in T1N affects the functions mediated by the two primary Orexin receptors, OX1R and OX2R:
| System Dysfunction | Receptor Focus & Function (Supported by sources) |
| Systemic/Autonomic Breakdown (OX1R) | Orexin-1 (OX1R) has high affinity for Orexin A and is concentrated in brain regions controlling non-wakefulness functions like feeding, memory, and reward [1]. The orexin neurons are an integral part of the central autonomic network [3]. |
| Sleep/Wake Regulation (OX2R) | Orexin-2 (OX2R) is primarily found in areas that regulate arousal [1]. This receptor is crucial for maintaining wakefulness, with the role of OX2R being considered more important than OX1R [1]. Research in mice demonstrates that those lacking the OX2R receptor show manifestations of narcolepsy syndromes [1]. |
T1N: The Systemic Breakdown
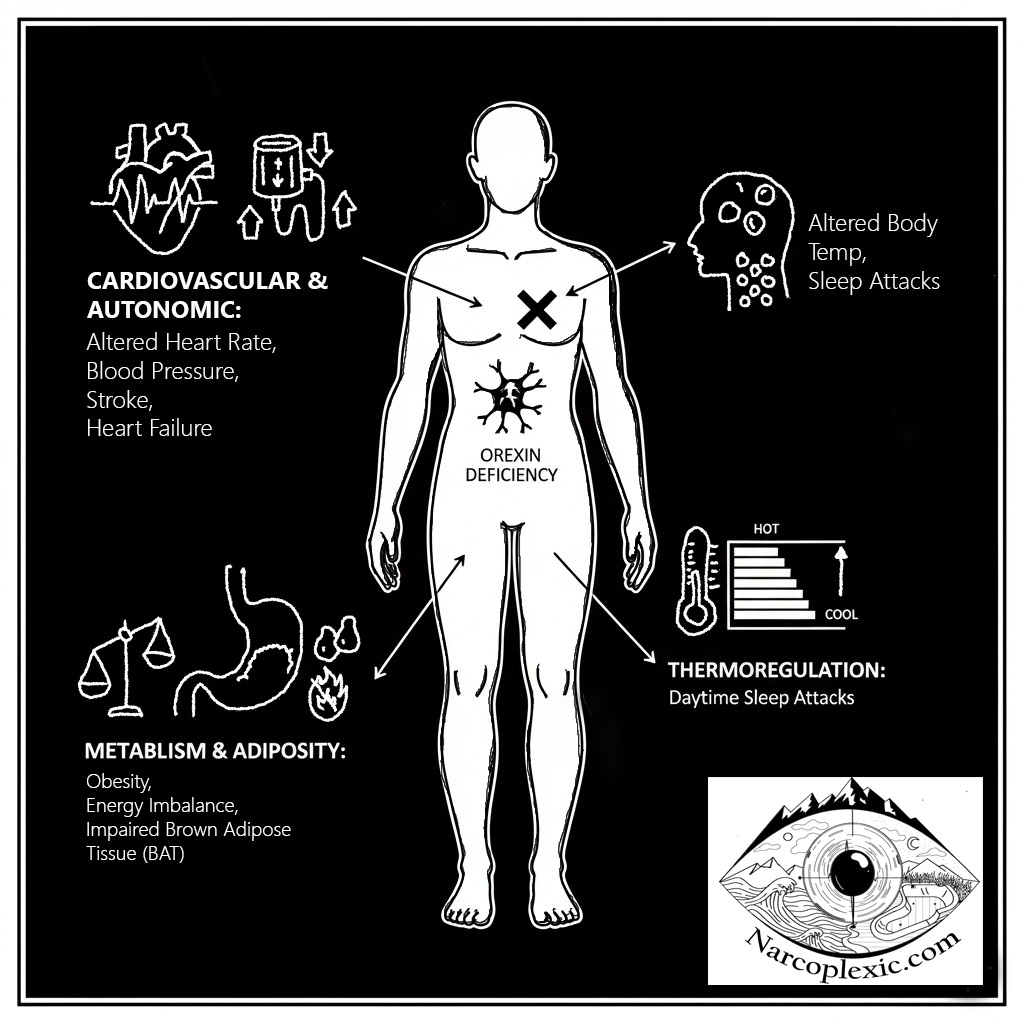
Orexin deficiency triggers measurable dysfunction across various bodily systems, there’s a reason those with T1N have a high rate of comorbidities [4][5] of all different sorts (the following are only a few examples of the directions they present in):
- Cardiovascular and Autonomic Systems: T1N is associated with autonomic nervous system dysfunction [3]. Patients show significant alterations in heart rate and blood pressure (BP) [3]. Compared to healthy controls, individuals with narcolepsy face a heightened risk of new-onset cardiovascular events [4], including stroke, heart failure, and major adverse cardiac events (MACE) [4]. The ability to achieve normal nocturnal BP dipping is often destabilized, as hypocretin is involved in regulating normal nocturnal blood pressure dipping, which can become dysregulated when hypocretin is deficient [4].
- Metabolism and Adiposity: Narcolepsy is linked to a significantly higher prevalence of obesity, despite patients often reporting normal or even reduced food intake [2][6]. This suggests an energy balance disruption, possibly involving lower basal metabolic rate [2][6].
- The orexin system is crucial for the development, differentiation, and function of Brown Adipose Tissue (BAT) [1][2][7], a highly metabolically active tissue involved in non-shivering thermogenesis [2]. Impaired BAT functionality resulting from the destruction of orexin-producing neurons is strongly hypothesized to contribute to the adiposity seen in T1N patients [2].
- Thermoregulation: Patients with T1N exhibit altered body temperature profiles [7]. They may have a higher core body temperature during the first part of the night compared to controls [7].
- Daytime sleep attacks are strongly predicted by physiological changes, specifically an increase in distal skin temperature and distal-to-proximal temperature gradient (DPG) in the minutes immediately prior to sleep onset [7].
The Psychological and Cognitive Toll
The debilitating nature of T1N results in an immense psychological and cognitive burden.
- Mental Health Comorbidities: There is a high co-morbidity with serious psychiatric conditions [5]. Depression is the most commonly reported psychiatric symptom [5], often linked to the chronic stress and impaired quality of life caused by the disorder, and is an independent risk factor for impaired quality of life [5]. Anxiety disorders, including panic attacks and social phobias, are also frequently reported, sometimes in as many as 53% of patients with narcolepsy [5]. High rates of psychiatric comorbidity are consistently reported in narcolepsy cohorts [3][5][8].
- Cognition and Attention: Cognitive deficits, often described as ‘brain fog’, encompass broad impairments in cognition, attention, and vigilance, significantly impacting daily function [5][9].
- ADHD: Symptoms of Attention-Deficit/Hyperactivity Disorder (ADHD) are reported at high rates in both pediatric and adult narcolepsy populations (up to two-fold higher than controls) [5]. Hyperactivity may, in some cases, be a compensatory response to being under-aroused or sleepy [5].
- Quality of Life: The chronic, debilitating reality of T1N [5], combined with the lack of truly restorative sleep, shatters the capacity to naturally recover and re-balance. This results in a heightened vulnerability to stress, significantly reduced quality of life [9], and an increased risk of mortality compared to those without narcolepsy [4][7].
Challenging the Clinical Focus
While drug development is crucial, the measure of therapeutic success must be scrutinized. If treatments, such as emerging orexin/hypocretin agonists [1], focus primarily on achieving extended wakefulness – merely keeping the eyes open – they may fail to address the core systemic dysfunction.
It is essential to prioritize treatments that promote systemic re-syncing and quality, restorative sleep. For instance, therapeutic agents like Sodium Oxybate (SXB) have shown evidence of addressing underlying dysfunction by improving nocturnal sleep [7] and successfully normalizing the core body temperature profile during the night to levels seen in controls [7].
To live with T1N is to constantly seek recognition for good reason, due to having a profound neurological failure that the world often minimizes. Accurate understanding of T1N as a major neurological system crisis is necessary to provide comprehensive support and appropriate treatment.
References
[1.]Xia L, Liu HY, Wang BY, Lin HN, Wang MC, Ren J-X. A review of physiological functions of orexin: From instinctive responses to subjective cognition. Medicine. 2023;102(26):e34206. [DOI] [PMC free article] [PubMed] [Google Scholar]
[2.]Straat ME, Schinkelshoek MS, Fronczek R, Lammers GJ, Rensen PCN, Boon MR. Role of Brown Adipose Tissue in Adiposity Associated With Narcolepsy Type 1. Front Endocrinol (Lausanne). 2020;11:145. [DOI] [PMC free article] [PubMed] [Google Scholar]
[3.]Silvani A. Autonomic nervous system dysfunction in narcolepsy type 1: time to move forward to the next level? Clin Auton Res. 2020;30:501–502. [DOI] [PubMed]
[4.]Ben-Joseph RH, Saad R, Black J, Dabrowski EC, Taylor B, Gallucci S, Somers VK. Cardiovascular Burden of Narcolepsy Disease (CV-BOND): a real-world evidence study. Sleep. 2023;46(10):zsad161. [DOI] [PMC free article] [PubMed]
[5.] Morse AM, Sanjeev K. Narcolepsy and Psychiatric Disorders: Comorbidities or Shared Pathophysiology? Med Sci (Basel). 2018;6(1):16. [DOI] [PMC free article] [PubMed] [Google Scholar]
[6.] Chabas D, Foulon C, Gonzalez J, Nasr M, Lyon-Caen O, Willer JC, Derenne JP, Arnulf I. Eating disorder and metabolism in narcoleptic patients. Sleep. 2007;30(10):1267–1273. [DOI] [PMC free article] [PubMed] [Google Scholar]
[7.] van der Heide A, Werth E, Donjacour CEHM, Reijntjes RH, Lammers GJ, Van Someren EJ, Baumann CR, Fronczek R. Core Body and Skin Temperature in Type 1 Narcolepsy in Daily Life; Effects of Sodium Oxybate and Prediction of Sleep Attacks. SLEEP. 2016;39(11):1941–1949. [DOI] [PMC free article] [PubMed] [Google Scholar
[8.] Xia L, Liu HY, Wang BY, Lin HN, Wang MC, Ren J-X. A review of physiological functions of orexin: From instinctive responses to subjective cognition. Medicine. 2023;102(26):e34206. [DOI] [PMC free article] [PubMed] [Google Scholar] [9.] Hlodak J, Geckova AM, Carnakovic S, Feketeova E. What is it like to live with narcolepsy? A scoping review. J Genet Med. 2025;29(1):93. [DOI] [PMC free article] [PubMed]
[9.] Hlodak J, Geckova AM, Carnakovic S, Feketeova E. What is it like to live with narcolepsy? A scoping review. J Genet Med. 2025;29(1):93. [DOI] [PMC free article] [PubMed]
Disclaimer: The information provided in this article is intended for informational and educational purposes only. Seek a qualified medical professional with expertise in Narcolepsy for diagnosis or treatment. I am not a medical professional.
Spanish version
Japanese/ソロモン・ブリッグスによる日本語訳
Created by: Solomon Briggs
(aka Narcoplexic)
October 21st, 2025
Type 1 Narcolepsy: A Neurological System Crisis, Not Just a Sleep Problem © 2025 by Solomon Briggs is licensed under CC BY-NC 4.0
To view a copy of this license, visit https://creativecommons.org/licenses/by-nc/4.0/
“You may use this tool for non-commercial purposes, but must credit Solomon Briggs.”